Michael Blaivas, J Ultrasound Med 2012; 31:823–826 |www.aium.org
During the last 20 years, ultrasound has been shown to be highly
effective in evaluating a range of pathologic pulmonary conditions. One of the
most widely studied and practiced applications is the evaluation of pneumonia
with ultrasound. Ultrasound interrogation of the thorax for detection of
pneumonia has been explored most in critical care and emergency department
settings. However, recently, the application has spread to general practice and
even prehospital settings. A number of scanning approaches exist, ranging from
highly involved research scanning tools to rapid and focused surveillance
scans. The most widely accepted protocol is performed rapidly and easily and
has proved to be sensitive and specific in adult and pediatric patients.
Multiple studies have shown lung ultrasound imaging to be more accurate than
chest radiography and in some cases rivals the accuracy of computed tomography
(CT), such as in the diagnosis of lung abscesses. This article reviews clinical
scenarios in which the lung ultrasound examination is useful in suspected
pneumonia, describes pathologic findings, and presents a commonly accepted
scanning protocol.
Overview and Clinical
Problem
The diagnosis of pneumonia, once thought to be accomplished simply by
physical examination, history taking, and specific auscultatory findings, has
recently become highly dependent on imaging. There is, in general, a method
behind this apparent clinical madness. Despite a long-held belief that physical
examination findings and proper auscultation are sufficient to rule in, or out,
the presence of pneumonia, multiple pressures in clinical practice have driven
increased use of chest radiography and occasionally CT. The physical
examination has proved to be unreliable for detection of pneumonia, even in
expert hands.1 Studies comparing
examinations by expert physicians to chest radiography have verified the
failure of auscultation as a diagnostic method in evaluation of pneumonia, yet
physicians are under an increasing burden to be more accurate, and missing
pneumonia is seen as a substantial liability. Additionally, the common approach
in general private practice of prescribing antibiotics to any patient
presenting with a cough and fever contributes to increasing antibiotic
resistance and is actively combated by the US Centers for Disease Control and
Prevention.
When faced with a patient with any combination of fever, cough,
shortness of breath, and hypoxia, clinicians think they have little option but
to obtain an imaging study or empirically prescribe antibiotics. In hospital
settings, patients may receive chest radiography routinely, not only for most
presentations to the emergency department with a cough but also in hospital
wards and intensive care units. In the latter two locations, chest radiography
may be a daily occurrence for some patients. However, one of the most clinically
frustrating aspects of searching for pneumonia with chest radiography is the
relatively low accuracy of this traditional imaging standby. Clinicians
frequently discover pneumonia on CT that was not seen on chest radiography
while searching for other pathologic conditions such as pulmonary embolisms.
Additionally, common chest radiography is associated with considerable
practical delays in most settings where a trained technologist obtains an image
and then processes it, both frequently away from the immediate clinical
setting. Point-of-care ultrasound imaging, performed at the patient’s bedside,
decreases the delays of chest radiography in diagnosis of pneumonia. Studies
showing the efficacy of lung ultrasound in detecting and ruling out pneumonia date
back approximately 20 years. Originally unrecognized by most in the medical
community, ultrasound imaging has proved superior to chest radiography in
almost every setting ranging from intensive care units to emergency departments
and outpatient clinics.2,3 The term “lung
ultrasound” is the most widely accepted one but is effectively equivalent to
“thoracic ultrasound” and “pleural ultrasound,” both of which have occasionally
been used in the literature.
Ultrasound Use
Performing the examination is easy and can be accomplished after
focused training. The original descriptions used a micro-convex ultrasound
transducer in the 5-MHz range. Little or no image postprocessing was available
at the time, and much of the science of lung ultrasound was built on artifacts
noted when the ultrasonic waves hit the pleural surface. In recent years, a
variety of ultrasound transducer types have been used to image the lung. The
most common, in addition to the micro-convex type, are linear and phased array
cardiac transducers, typically ranging from 10 to 5 and 5 to 2.5 MHz,
respectively. The linear arrays, much like a curved linear abdominal probe,
have difficulty getting in between ribs, substantially limiting imaging in some
patients. However, the pleura and near-pleural abnormalities are seen much
better than with the micro-convex and phased array transducers, which are
probably best suited for general lung applications such as pneumonia screening
in most patients. In the adult patient, the field depth is typically set at 16
to 18 cm, commonly found on most machine presets. Image postprocessing settings
such as tissue harmonics and multibeam functions are best turned off if
possible. Such settings may eliminate artifacts and could impede diagnosis. The
ultrasound transducer is moved until a rib interspace is located. The probe is
then panned horizontally and vertically to the extent possible to allow the
broadest sweep through the area being imaged. The transducer indicator is
pointed cephalad and then to the patient’s right, allowing for the best
ultrasound penetration between ribs. Holding the transducer perpendicular to
the chest wall and panning of the beam are accomplished with subtle movements
and angle variations. For the most consistent and accurate results, the
operator should use a methodical scan to map out the entire thorax. The
micro-convex and phased array transducers are ideal for manipulating the
ultrasonic beam in the rib interspaces. One exception is the young pediatric
patient, for whom linear array or high-resolution micro-convex transducers are
best suited to the small body size.

Figure
1.
The scanning position for the lateral chest is shown. A phased array
cardiac transducer was used for this 8-point pneumonia survey.
When evaluating for pneumonia, the ultrasound transducer is typically
applied to 4 different windows on each hemithorax. In a reclined or
semireclined patient, the 8 regions include the upper and lower regions of the
anterior hemithorax and upper and lower regions of the lateral hemithorax (Figure 1). An
entire region is surveyed by angling and sliding the ultrasound transducer as
needed. The pleural surface of the lung acts as an acoustic reflector,
reflecting nearly 80% of the ultrasonic beam it encounters. As seen with other
anatomic structures with high impedance, horizontal reverberation artifacts are
readily created and are known as A-lines in the lung ultrasound lexicon (Figure 2). The
healthy, well-aerated, and inflated lung has a density of approximately 0.32
g/mL and is not acoustically penetrated by medical ultrasound to an appreciable
degree.4 When the fluid
content of the lung increases, substantial impedance differences are
encountered in close proximity, leading to generation of additional artifacts
termed B-lines, which are frequently seen in pulmonary edema. These artifacts
are classically described as discrete laser-like vertical hyperechoic entities,
which appear to arise at the pleural line and extend to the bottom of the
ultrasound image without fading. Debate still exists about their exact source.
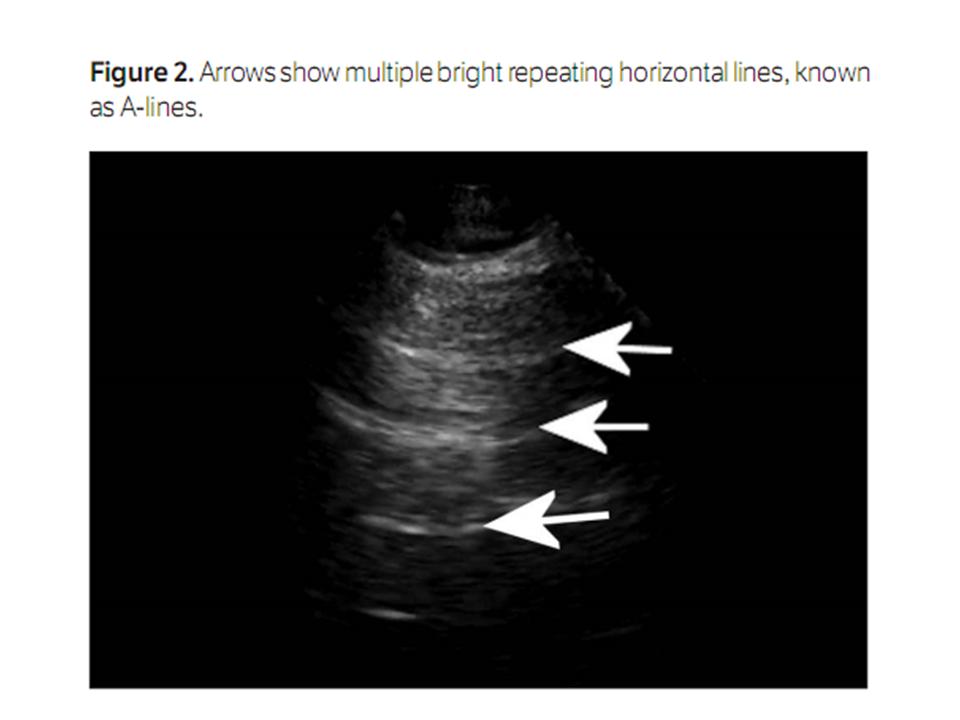
Figure
2.
Arrows show multiple bright repeating horizontal lines, known as
A-lines.
The key to ultrasound visualization of pneumonia in the lungs is
relative loss of aeration of a portion of the lung and a concomitant increase
in the fluid content, which is seen in lung consolidation. Once this
consolidation reaches the pleura, it can be seen with ultrasound. Although some
very early pneumonias must be so localized as to not abut the lung pleura, most
make contact at some point inside the chest in clinically symptomatic patients
and can thus be imaged with ultrasound. Current literature suggests that most
pneumonias in critically ill patients (up to 98%) will contact the pleura.5 On a standard
ultrasound examination, lung consolidation from pneumonia is often described as
having a tissue-like pattern and is referred to as “hepatization” to illustrate
its gray scale density and general appearance (Figure 3).
Boundaries of a consolidated lung segment are defined by the pleural line, the
adjacent aerated lung, and any effusion that may be present. The boundary
created by adjacent aerated lung will naturally appear irregular. An exception
is when an entire lobe is affected, in which case the boundary will be regular
and well defined. A dendrite-like air bronchogram and a large number scatter
artifacts from air are frequently traceable up to the pleura (Figure 4). In real
time, air can be seen moving through bronchi, and this finding is known as a
dynamic air bronchogram (Video 1). On color or power Doppler imaging, vascular
flow in cases of pneumonia is seen as a classic branching pattern in the
infected/consolidated lung. Table 1 summarizes
the typical ultrasound findings associated with pneumonia.

Figure
3.
This image shows a solid organ–appearing structure in the near field.
In actuality, the scan was performed through the lateral thorax. The lung is
consolidated in a case of pneumonia and has an echo texture similar to that of
the liver (Lung). Adjacent to it, the heart is shown, which is not possible
through healthy lung. Several vessels are shown near the heart with a great
vessel (GV).

Figure
4.
This image shows air bronchograms. The liver is shown on the right side
of the screen with the diaphragm just to the left. The content of the thorax
above the diaphragm is easily visualized (Lung) and appears to have a
liver-like echo texture. Arrows point to bright branching signals within the
consolidated lung, which represent the air bronchograms.
The sensitivity of B-mode ultrasound imaging is about 90%.5 Consolidation and
dynamic air bronchograms have the highest specificity for pneumonia. Several
studies showed that ultrasound imaging outperformed chest radiography with CT
of the chest as a reference standard.2,6–10 Interestingly,
lung ultrasound has grown to such an extent that an evidence-based consensus
conference was held in 2010 and 2011, grading supporting evidence and bringing
together dozens of published experts from multiple countries around the world.11 The consensus
conference found lung ultrasound to have broad utility in evaluating patients
for pneumonia, lung contusions, pneumothorax, pulmonary edema, pulmonary
embolisms, and other pathologic conditions. In general, ultrasound imaging
performed better than plain radiography.

Table
1.
Most Common Ultrasound Findings Associated With Pneumonia
Discussion
Lung ultrasound imaging for the detection of pneumonia is highly
accurate but like most diagnostic tests is not perfect. It is important for the
sonologist to realize that lung consolidation can result from several different
pathologic conditions. These include not only pneumonia but also acute
respiratory distress syndrome (ARDS), lung contusions, and atelectasis.
Although differentiating between pneumonia and atelectasis is probably the most
difficult on the basis of clinical grounds, it is easily accomplished with
ultrasound. Atelectatic lung segments (clinically the most commonly encountered
mimickers) will show the absence of regional blood flow in the affected area of
the lung on color or power Doppler interrogation. Patients with ARDS and lung
contusions are often obviously clinically but will show the presence of blood
flow on Doppler imaging. Lung contusions are typically encountered in patients
with blunt trauma and will show abolishment of lung sliding; in some cases,
they have even been mistaken for pneumothorax. However, contusions will also
show localized signs of pulmonary edema and asymmetry between the left and right
lungs, which can help differentiate them from pneumonia. On the other hand,
ARDS will almost always show pleural line irregularities and will frequently
show subpleural consolidation. These signs can allow clinicians to distinguish
between major causes of lung consolidation on ultrasound imaging. As with any
ultra-sound application, operator competency is critical, and error can occur
if the operator is not properly trained and experienced. Fortunately, it
appears that lung ultrasound imaging has a favorable learning curve. However,
misdiagnosis of pneumonia or, worse, failing to detect pneumonia could
negatively affect the patient.
The use of lung ultrasound in the evaluation of pneumonia is growing
rapidly and in each clinical setting shows increased efficiency as accurate
bedside diagnosis is made possible. Although many traditional imaging
applications are still indicated and will be used indefinitely for patients
with possible pneumonia, lung ultrasound can substantially decrease the
practical delays associated with plain chest radiography and in some cases can
obviate the need for chest CT when a definitive diagnosis is obtained on
ultrasound imaging, avoiding a large radiation dose. In many cases when
pneumonia is in the differential diagnosis, lung ultrasound should come first.
Footnotes
The Sound Judgment Series consists of invited articles highlighting the
clinical value of using ultrasound first in specific clinical diagnoses where
ultrasound has shown comparative or superior value. The series is meant to serve
as an educational tool for medical and sonography students and clinical
practitioners and may help integrate ultrasound into clinical practice.
Không có nhận xét nào :
Đăng nhận xét