



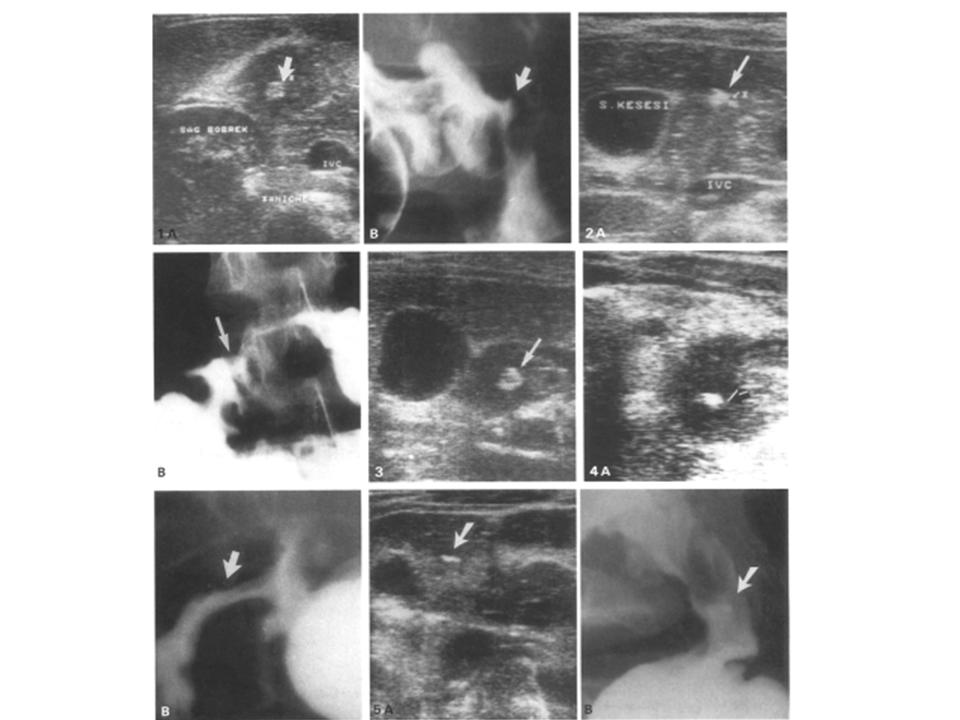
Fig. 1. Case 1. A Transverse sonogram demonstrates an echogenic core surrounded by a thick hypoechoic halo lateral to head of the pancreas (arrow). B Ulcer and spasm at the apex of duodenal bulb (arrow).
Fig. 2. Case 2. A An irregular echogenic area surrounded by a hypoechoic rim between gallbladder and head of the pancreas (arrow). B Barium collection and bulber deformity due to duodenal ulcer (arrow).
Fig. 3. Case 3. Sonogram demonstrated a hypoechoic solid mass with a central echogenic area adjacent to gallbladder (arrow). Follow-up UGI series in the prone position showed a large ulcer in the postpyloric area.
Fig. 4. Case 4. A An echogenic area surrounded by a thick hypoechoic rim (arrow). B Severe deformity of duodenal bulb due to chronic peptic ulcer is visible on UGI exam (arrow).
Fig. 5. Case 5. A Linear echogenic appearance adjacent to gallbladder. Duodenal wall is thickened (arrow). After some water administration, linear echogeneity was seen in the anterior duodenal wall as a mucosal defect. B The x-ray demonstrates a linear ulcer in the duodenal bulb (arrow).
Discussion
Abdominal US is becoming more frequently used as a primary screening procedure for the evaluation of nonspecific abdominal complaints. Since barium is highly reflective to ultrasound, US is often performed before UGI series. Bowel lesions may therefore be encountered during the US examination. Occasionally, US will permit characterization of a bowel lesion even when it cannot be established radiologically.
The US patterns of normal bowel are variable, depending upon the intraluminal contents. Bowel may be either collapsed or contain varying quantities of fluid and gas. An US pattern consisting of a rounded mass with an echogenic core and a sonolucent halo (target or "bull's-eye" configuration) is commonly encountered on abdominal US arising from a collapsed mucus-filled bowel.
A similar configuration can be observed emanating from a variety of benign and malignant bowel lesions such as congenital pyloric stenosis, intramural hematomas, inflammatory bowel disease especially Crohn's, ileocecal tuberculosis, acute appendicitis, edema of the intestinal wall secondary to thrombosis of the mesenteric veins, Menetrier's disease, ischemia, diverticular disease, and bowel neoplasms [8-11]. However, the target configuration originating from bowel lesions has a hypoechoic halo that is abnormally thick and an echogenic core that is eccentrically located. This appearance has been given US descriptions: the cockade sign, the pseudokidney sign, or the abnormal target appearance [1, 8, 12]. Peristalsis will be absent or diminished, as observed with real-time scanning in affected bowel segment [12].
Echogenic cores in my cases are compatible with ulcer findings in x-rays, according to their shape, volume, and localization. This echogeneity might well result from necrotic fibrinoid debris covering the surface of the niche as a thin layer.
The hypoechoic halo around it might be a counterpart of wall edema and/or infiltration often produced during the active inflammatory phase of duodenal peptic ulcer. Epigastric pain that has been observed as the main complaint in all cases is a significant symptom supporting that the ulcer is in an active phase.
Relatively few reports have been published about US appearances of gastric and duodenal ulcers [2-7]. A case of large gastric ulcer presented with thickening of the gastric wall on US [1]. In another case of antral ulcer demonstrated by a UGI series, the hyperechoic core with an acoustic shadow surrounded by a hypoechoic halo was the US findings of an ulcer niche on the posterior antral wall [2]. Multiple gastric ulcers in a child were demonstrated as a mucosal defect on the thickened antral wall and their response to therapy was followed with US [3]. The appearances of my 5th case, which showed a mucosal defect on the thickened anterior wall of the duodenum, is very similar to this case.
Publications about US appearances of duodenal peptic ulcers are still few [7]. In one study, US appearances of 2 giant peptic ulcers are defined as cystic cavity. In 1 of these 2 cases, an echoic appearance surrounded by a hypoechoic rim, which is very similar to my cases, was defined as the thickening of the duodenal wall [6]. This appearance, however, may represent the ulcer while the cystic area adjacent to it might possibly be a pseudodiverticulum.
Gas in the lumen of the GI tract prevents US examination. When a duodenal peptic ulcer is in an acute inflammatory phase and accompanied with spasm, the collapse of the lumen eliminates gas accumulation. The use of excellent acoustic windows such as the liver and gallbladder is an important factor enabling us to study the duodenum without gas in the lumen. If an ulcer is located on the anterior wall of duodenum, even an open lumen will not prevent the demonstration of ulcer as in the 5th case. In conditions like acute appendicitis, intestinal wall thickening is easily recognized by ultrasonography. With probably more prominent wall thickening, mucosal changes of niche, and good acoustic windows, the acute duodenal ulcer should be expected to be more detectable than acute appendicitis.
In conclusion, the initial diagnosis of a duodenal peptic ulcer in the acute phase may first be indicated by the ultrasonologist. Further studies, especially correlated with duodenoscopy, are necessary to establish the role and importance of US in duodenal ulcer diagnosis.
Không có nhận xét nào :
Đăng nhận xét