ABSTRACT
Point-of-care ultrasound (POCUS) has become a reliable and powerful tool working as a complement to the traditional physical examination. It has proven to be a reliable and reproducible method to a quicker and safer diagnosis, sometimes surpassing the diagnostic accuracy of more traditional techniques. We present two cases of pulmonary embolism (PE) with clinical presentations that suggested other diagnoses, prior to the performance of POCUS: a 60-year-old patient with nausea and vomiting and a 66-year-old female with a week-long progressive increase of shortness of breath and increased peripheral edema. In the reported cases, we aim to pinpoint the importance and usefulness of POCUS in the everyday evaluation of our patients, in multiple settings and by multiple specialty physicians, supported by its robust evidence-based background. It has proven to be a useful tool in evaluating in a fast and nonharmful way complementing more traditional techniques, which proves to be especially important regarding cases, like the ones we describe, when the correct diagnosis is not always clear to presentation. The use of multiorgan POCUS allows even in the most atypical presentations, the rise of suspicion of PE, leading to the necessary steps to a final diagnosis and management.
Keywords: Deep vein thrombosis, lung ultrasound, point-of-care ultrasound, pulmonary embolism
Keywords: Deep vein thrombosis, lung ultrasound, point-of-care ultrasound, pulmonary embolism
DISCUSSION
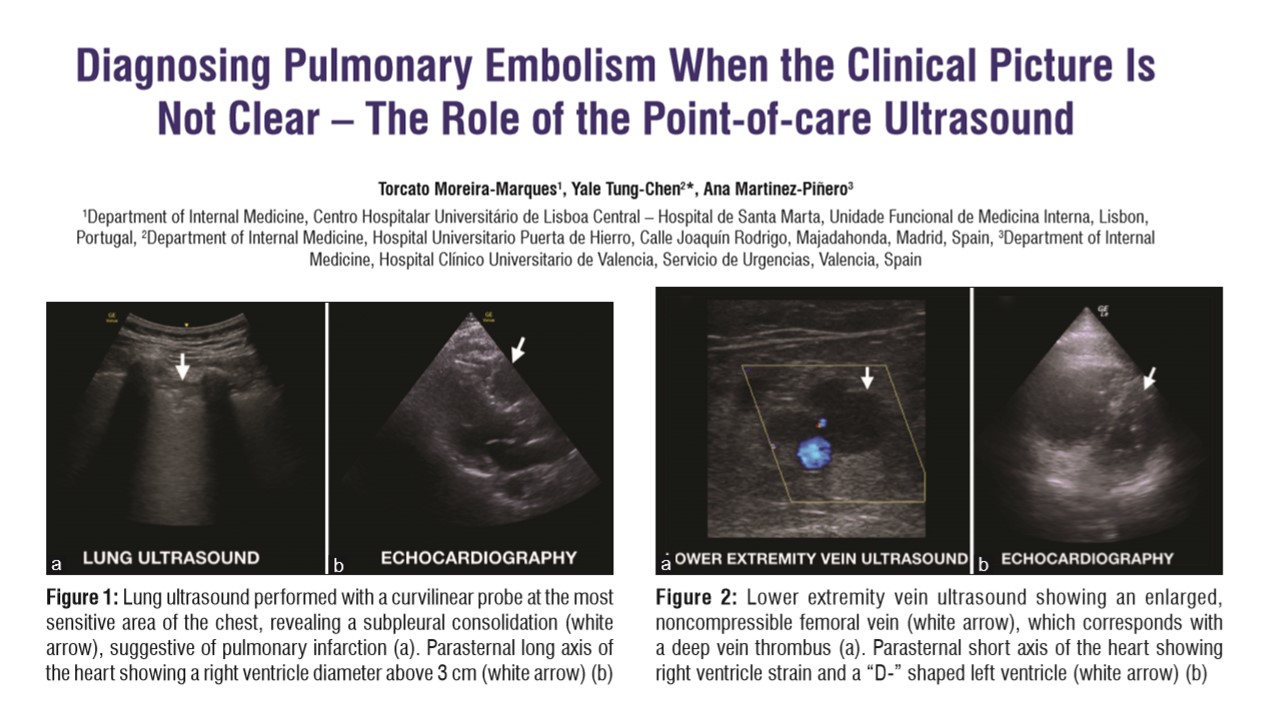
Multiorgan POCUS has a robust evidence-based background. It is adopted by a variety of physicians in a lot of different settings, allowing to a more efficient and quickly evaluation and management of our patients.[2,3] This way, it proves to be highly valuable as a complement to traditional examination tools, especially when it comes to cases where the clinical picture is unclear. Regarding PE, the range of presentations is wide,[4] frequently leading to misdiagnosis and otherwise preventable morbidity and death.[5] Atypical presenting symptoms of PE, such as syncope, recurrent fever,[6] bradycardia,[2] epigastric pain,[7] flank pain,[8] right upper quadrant and back pain,[9] and seizure,[10] are described in the literature despite their rarity. This leads to the need of a more cautious approach in patients with risk factors for PE despite their presentation.[4] The value of POCUS stands out in these cases, especially in a multiorgan approach.[2] Multiorgan POCUS including lung, venous compression, and focused cardiac ultrasound as a clinical adjunct can play a significant role in the diagnosis and management of PE. The presence of subpleural consolidations and focal B-lines is highly specific for focal interstitial syndrome (i.e., pneumonia, fibrosis, atelectasis, pulmonary infarction, neoplasia, etc.). Compression ultrasound is the mainstay of venous thrombosis diagnosis. Focused cardiac ultrasound may reveal evidence of right ventricle strain. Combining these examinations in a protocolized approach allows a quick but unrefutably precious look at the most important locations regarding PE.[2] POCUS is useful in the diagnosis of acute PE, either as a screening tool in patients with atypical presentation or as an aid before the confirmation by chest computed tomography in patients with high clinical suspicion, leading to the necessary steps to a final diagnosis and management.
We have obtained informed consent from the patients.
Không có nhận xét nào :
Đăng nhận xét