
IBD is one of the most common gastrointestinal diseases affecting pediatric patients in the developed world [1]. Crohn disease (CD) and ulcerative colitis (UC) are the two predominant subtypes of IBD, differing both in distribution of gastrointestinal tract involvement and depth of inflammation. Both disorders are most common in Europe and North America, where the ranges of incidence and prevalence are 3.1–14.6 cases per person-years and 26–199 cases per 100,000 persons for CD and 2.2–14.3 cases per 100,000 person-years and 37–246 cases per 100,000 persons for UC [1]. The classic teaching is that CD has a bimodal peak—the first peak in the second or third decade of life and a smaller second peak in the sixth or seventh decade. There is equal evidence, however, of a unimodal peak in the second or third decade that explains the high incidence in the adolescent population [1, 2]. CD is more common than UC among adolescents, and adolescents with UC tend to have more severe and extensive disease at presentation than their adult counterparts do: Approximately 90% of adolescents present with total colonic involvement [3]. Because the bowel disease in UC is confined to the colon, total colonic surgical resection is curative for patients whose condition is refractory to medical therapy. In contrast, the potential involvement of the entire gastrointestinal tract in CD often leads to lifelong intermittent symptomatic recurrence, and medical rather than surgical management is the primary therapy. No consensus exists regarding the optimal technique and imaging modality for evaluating IBD. The choice of imaging is informed by the clinical presentation of the patient. The choice of specific modality is based on the need to assess the distribution or activity of the disease and to detect extraluminal complications, such as intraabdominal abscess, perforation of bowel, and enteric fistula. Pediatric patients need additional attention to minimization of radiation exposure during imaging examinations because the chronic remitting and relapsing nature of IBD, especially CD, frequently necessitates repeat imaging with a resultant greater cumulative lifetime radiation exposure.

Ultrasound has the advantage of being a noninvasive test
that imparts no ionizing radiation. High interoperator variability, however, is
a practical consideration for determining its true diagnostic accuracy.
Targeted assessment of the bowel wall is usually performed
with a high-frequency linear-array probe. As with fluoroscopy, with ultrasound,
bowel loops can be observed over time for evaluation of peristalsis and
function.
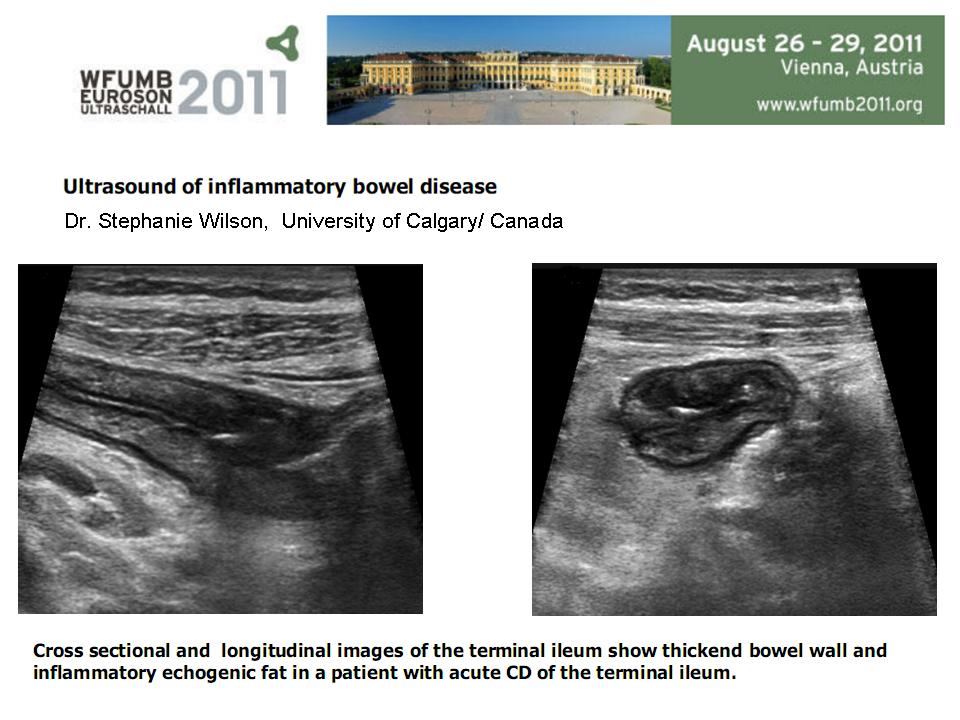
The ultrasound criteria for assessment of CD include
assessment of wall thickness, loop stiffness, bowel dilatation, presence or
absence of strictures, abnormal peristalsis, presence of fistula or
abscess, and mesenteric inflammatory change. A previous meta-analysis
revealed mean per patient sensitivity of 89.7% and specificity of 95.6% and per
bowel segment sensitivity and specificity of 73.5% and 92.9%. Patient
preparation is not usually required, although the studies are usually performed
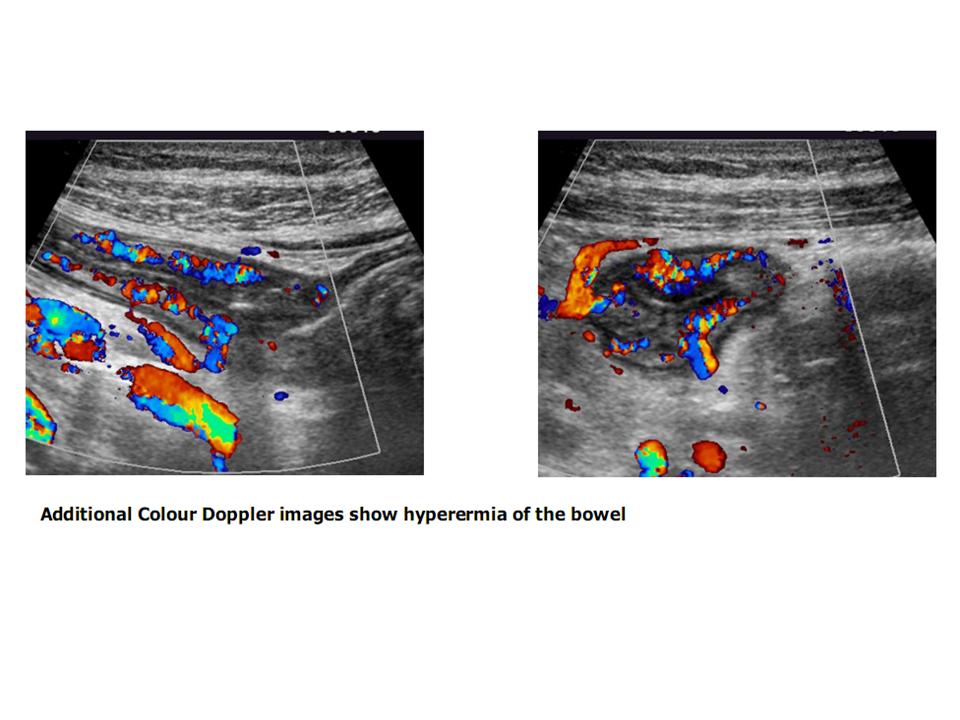
after the patient has fasted. Use of contrast material has been found to
increase accuracy, and Doppler evaluation of bowel wall vascularity may help to
determine the presence of disease activity or quiescence.
Poor visualization of the rectum and sigmoid colon, owing to
the location of these structures in the pelvis, makes ultrasound less suitable for
assessment of UC. The spatial resolution of ultrasound also is lower than
that of barium studies.
In all of the ultrasound studies, wall thickness was the
principal imaging parameter. The sensitivities and specificities were consistently
much lower than with the cross-sectional modalities; the range of sensitivity
was 0.48–0.8 and that of specificity was 0.57–0.93 across the three papers.
Ultrasound yields useful information on bowel wall
abnormalities and can be accurate in experienced hands; however, because of low
sensitivity and specificity and high interoperator variability, ultrasound is
not recommended for first-line imaging in the three clinical scenarios posed.
The Three Typical Clinical Scenarios
1/ Pediatric patient: initial diagnosis of suspected
inflammatory bowel disease, differentiation of Crohn disease from ulcerative
colitis.
2/ Pediatric patient: known inflammatory bowel disease with
new acute presentation (fever, peritonitis, leukocytosis).
3/ Pediatric patient: known inflammatory bowel disease with
symptomatic recurrence (abdominal pain, diarrhea), not acutely ill.
Xem SIÊU ÂM TRONG BỆNH LÝ VIÊM RUỘT (IBD)
Xem SIÊU ÂM TRONG BỆNH LÝ VIÊM RUỘT (IBD)




