

Abstract
Histotripsy is the first noninvasive, non-ionizing, and non-thermal ablation technology guided by real-time imaging. Using focused ultrasound delivered from outside the body, histotripsy mechanically destroys tissue through cavitation, rendering the target into acellular debris. The material in the histotripsy ablation zone is absorbed by the body within 1–2 months, leaving a minimal remnant scar. Histotripsy has also been shown to stimulate an immune response and induce abscopal effects in animal models, which may have positive implications for future cancer treatment. Histotripsy has been investigated for a wide range of applications in preclinical studies, including the treatment of cancer, neurological diseases, and cardiovascular diseases. Three human clinical trials have been undertaken using histotripsy for the treatment of benign prostatic hyperplasia, liver cancer, and calcified valve stenosis. This review provides a comprehensive overview of histotripsy covering the origin, mechanism, bioeffects, parameters, instruments, and the latest results on preclinical and human studies.

The University of Chicago Medicine was the first health system in Illinois to treat patients with histotripsy, a new noninvasive technology that uses ultrasound energy to precisely destroy liver tumors.
UChicago Medicine has been involved for years in bringing histotripsy to patients, having treated patients in the US arm of the #HOPE4LIVER clinical trial. Histotripsy technology received FDA approval in October 2023, and UChicago Medicine physicians expect to begin clinical implementation in early 2024.
Safely Destroying Tumors With Targeted Sound Waves
Histotripsy technology uses high-intensity sound waves to selectively destroy cancer tissue in the liver. Unlike traditional methods such as surgery, radiation, or ablation, the procedure does not require any incisions, radiation, needles, or invasive procedures.
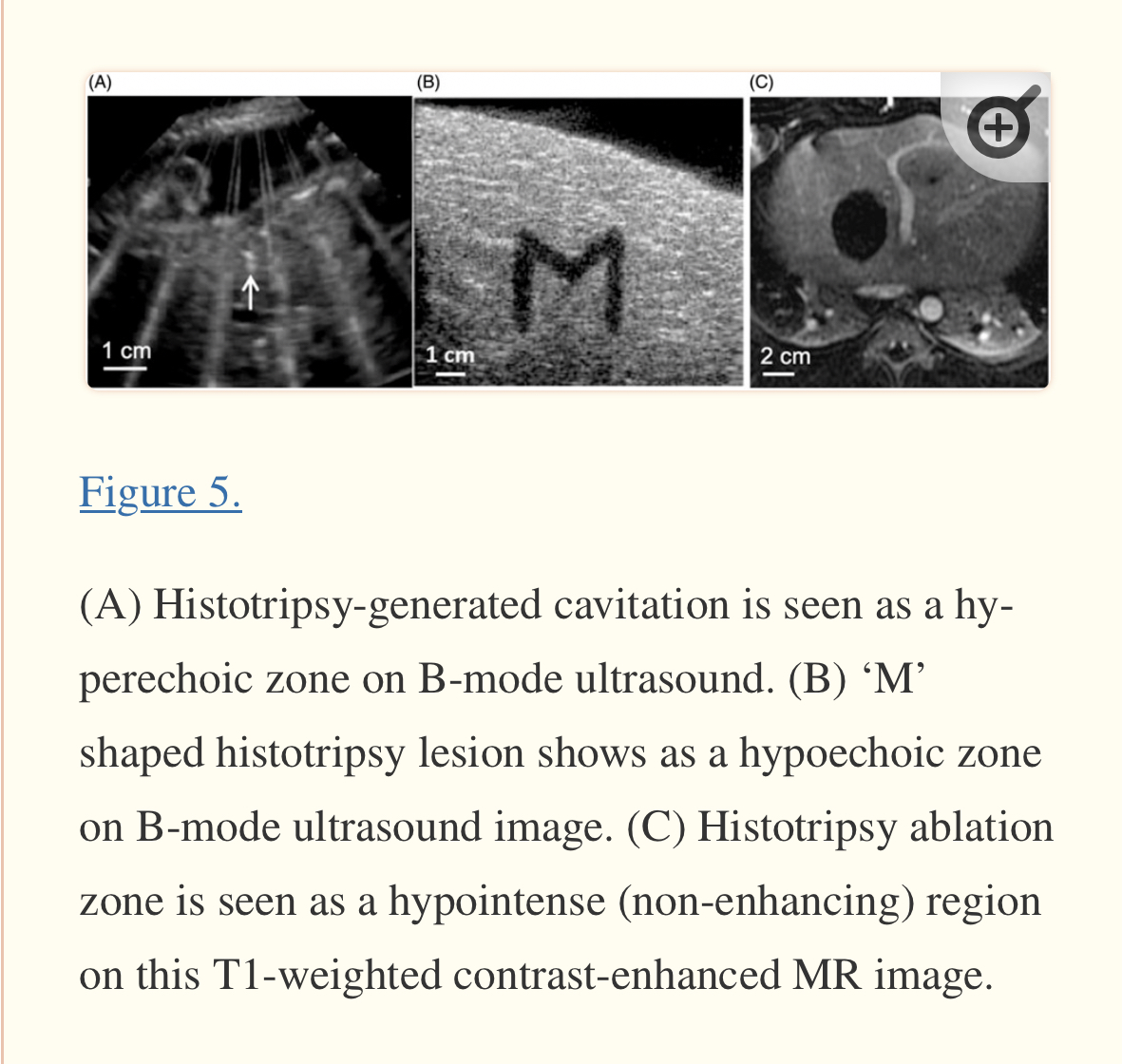
Before histotripsy treatment, doctors use ultrasound imaging – like what is used to see babies in the womb – to locate the tumor, determine the size of the area that needs to be treated, and target and monitor the treatment area during the procedure. After doctors program the histotripsy robot with the tumor’s coordinates, the machine precisely generates focused sound waves that create a "bubble cloud" inside the targeted area, which disrupts and destroys only the cancerous tissue.
“One of the best things about how this technology works is that it’s protective of things we don’t want to damage,” said Osman Ahmed, MD, associate professor of radiology at UChicago Medicine. “A histotripsy procedure can damage or kill a tumor while leaving important structures like blood vessels and bile ducts intact.”
The treatment is so simple and noninvasive that Ahmed said patients can even wear a t-shirt and jeans rather than a surgical gown.
“The actual procedure can take 5 to 30 minutes depending on the size of the tumor,” he said. “Then we move the robot away, and the patient wakes up. They can even go home the same day unless they have pain.”